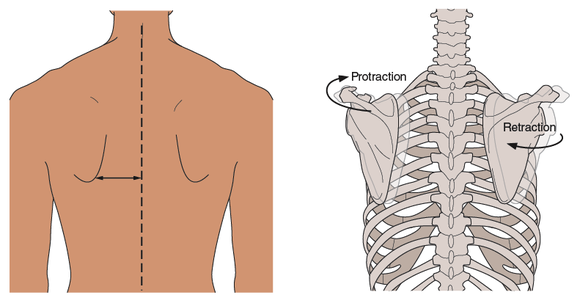
Step 7 Scapular Adduction and Abduction
Next, take a look at the scapulae and their relationship to the client’s spine. Observing the relationship between the medial borders of the scapulae and the spine, decide whether the scapulae are adducted (retracted) or abducted (protracted). Many clients, unless engaged in regular exercise or sporting activity involving the upper body, have slightly protracted scapulae. This could be due in part to the kyphotic posture many people adopt when sitting.
TIP If you cannot see the medial border, gently palpate for it. To locate it, ask your client to place his hand behind his back while you do this. Remember that, in doing so, the scapula will change position. You may find that drawing a horizontal line on the skin directly down this border helps you get a better idea of the position of the scapulae.
What Your Findings Mean
Protraction of the scapulae often accompanies poor posture in which the rhomboids and the lower fibers of the trapezius are lengthened and weak bilaterally. Retraction of the scapulae is much less common and occurs when people adopt a military-style posture: chests pushed up and out, shoulders drawn back and down. In this case rhomboids might be shortened on both the left and right sides of the body. Clients engaged in sporting activity in which retraction predominates on one or both sides of the body (e.g., javelin throwers and archers) might demonstrate unilateral shortness in the rhomboids on the side of the retraction. Observation of clients who regularly engage in sporting activities involving bilateral retraction of the scapulae—such as rock climbing and rowing—may reveal hypertrophy in both left and right rhomboids.
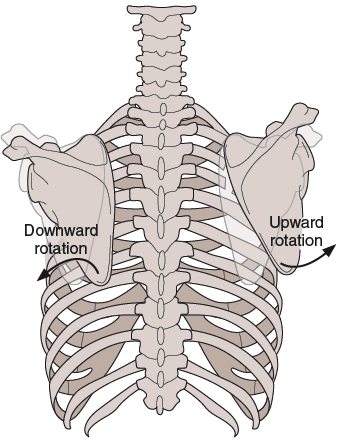
Consider, also, what happens to the medial border when the scapulae rotates. With upward rotation the medial border and inferior angle are abducted from the spine, lengthening the rhomboid major and shortening the rhomboid minor and levator scapulae. With downward rotation, the medial border and inferior angle are adducted towards the spine, shortening the rhomboid major and lengthening the rhomboid minor and levator scapulae. Table 3.1 summarises this information. Notice that the serratus anterior has been included in this table because it attaches to the medial border of the scapulae on the anterior surface of the bone. For more information about rotation of the scapula, see step 9.
When assessing the shoulder region, as with any area of the body, be careful not to jump to conclusions regarding the source of shoulder pain. Just because a person stands with protracted scapulae and an internally rotated humerus, for example, does not mean that her scapular pain results from the anatomical positions of these bony structures. There are other possible sources of pain. For example, way back in 1959, Cloward reported on the likelihood of scapular and upper limb pain originating from cervical discs.
  | |
Read more from Postural Assessment by Jane Johnson.
|
суббота, 28 декабря 2013 г.
Assessing posture through scapular adduction and abduction
Подписаться на:
Комментарии к сообщению (Atom)
Комментариев нет:
Отправить комментарий