How many times have we done or seen people at the gym doing the “wind-mill” stretch before a workout? Sooner or later every weightlifter will experience pain and tenderness in their shoulder. The pain usually lingers for weeks if not months, and the pain is usually more noticeable when performing a bench and/or overhead press, but it gets better later into the workout. Chances are someone has said that it is possibly bursitis or rotator cuff issue, and rest and “take it easy” is the best way to treat it, but taking it easy or rest isn’t going to happen.
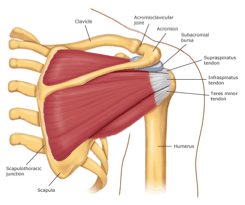
Most of the time when someone comes into my office with shoulder pain, it is caused by impingement syndrome. Impingement syndrome occurs when the tendons of the rotator cuff muscles become irritated and inflame as they pass through the subacromial space. This results in pain, weakness, and loss of movement at the shoulder joint1. Some of the causes are2:
• Keeping the arm in the same position for a long period of time.
• Sleeping on the same arm each night.
• Overhead sports like tennis, baseball (especially pitching), swimming, and weight lifting.
• Overhead jobs like painters.
• Poor control or instability of the shoulder muscles.
• Sleeping on the same arm each night.
• Overhead sports like tennis, baseball (especially pitching), swimming, and weight lifting.
• Overhead jobs like painters.
• Poor control or instability of the shoulder muscles.
Early on the pain usually only happens with overhead activities and lifting the arm. Over time, the pain may start happening at night, especially when laying on the involved side. Pain is usually located in the front of the shoulder and may radiate to the side of the arm. If the pain radiates past the elbow, it might be due to a pinched nerve. The best way to diagnose impingement is through history and orthopedic testing. Some of the details that should be made available to your doctor when evaluating possible shoulder impingement include any history of previous trauma, positions that aggravate the pain, and what makes it better or worse. Another important factor to consider is how it affects your daily activities and workouts. What exercises are the worst to perform? Do you train your other muscles of the shoulder? If so, how often? Answering these questions will help your doctor to provide the correct diagnosis and the best course of action.
If you are suffering from impingement of the shoulder, the best thing to do is to rest, and stop all activities that will aggravate the shoulder. The pain and inflammation can be reduced through the use of therapeutic modalities like ice, ultrasound, and electrical stimulation, and through the use of nonsterodial anti-inflammatory drugs (NSAIDS)3. Manual therapies such as Active Release Technique, FAKTR-ISTM, and/or Gratson Technique also help in reducing inflammation. For severe cases, a corticosteroid injection may be necessary to relieve discomfort. A stretching program should also be implemented to increase flexibility. Stretching should include the posterior shoulder, the pectoralis minor, triceps, and biceps3. The Sleeper Stretch is an excellent stretch for impingement.
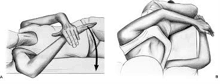
Sleeper Stretch
When performing a sleeper stretch, make sure that you are not laying flat on your scapula, you want to lay mostly on your rib cage and the outside border of your scapula. Your arm should be 90 degrees from your torso with the palm of your hand facing the ground. Then you want to gently push down at your wrist until you feel a mild stretch on your posterior shoulder and hold for 30 seconds. Do this for about 3 reps. You should not feel anything in the front of your shoulder, and be careful to not push too hard. With this stretch your hand is not supposed to touch the ground. The goal is to feel a mild stretch in the back of the shoulder and hold the position4.
Rest and avoid overhead workouts are the best way to treat impingement syndrome, along with regular stretching, and myofascial release techniques the symptoms should alleviate sooner. Remember, if you are experiencing pain, seek the help of a health care specialist; it won’t just “go away”.
In the next article I will talk about some exercises to mix into the shoulder routine to prevent impingement from happening.
PART TWO HERE
1. Fongemie AE, Buss DD, Rolnick SJ. (1998). Management of Shoulder Impingement Syndrome and Rotator Cuff Tears”. American Family Physician 57: 667–74, 680–2.
2. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001474/
3. Kirchhoff, Choldwig., Imhoff, Andreas B. (2010) Posteriosuperior and anterosuperior impingment of the shoulder in overhead athletes – evolving concepts”. International Orthopaedics. 34(7): 1049-1058.
4. Laudner, Kevin G PhD, ATC., Sipes, Robert C, ATC, CSCS., Wilson, James T, ATC, CSCS. (2008). The Acute Effects of Sleeper Stretches on Shoulder Range of Motion. Journal of Athletic Training. 43(3): 359-363.
2. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001474/
3. Kirchhoff, Choldwig., Imhoff, Andreas B. (2010) Posteriosuperior and anterosuperior impingment of the shoulder in overhead athletes – evolving concepts”. International Orthopaedics. 34(7): 1049-1058.
4. Laudner, Kevin G PhD, ATC., Sipes, Robert C, ATC, CSCS., Wilson, James T, ATC, CSCS. (2008). The Acute Effects of Sleeper Stretches on Shoulder Range of Motion. Journal of Athletic Training. 43(3): 359-363.
Комментариев нет:
Отправить комментарий