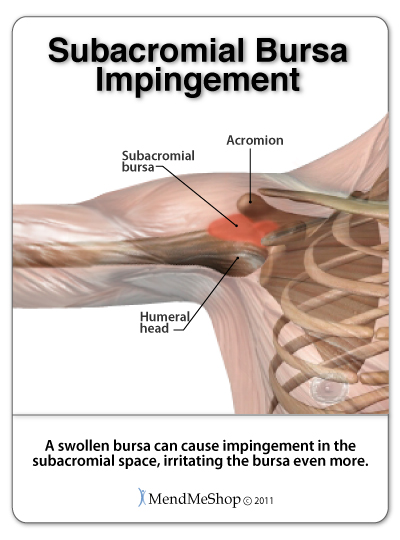
Shoulder impingement syndrome occurs when soft tissue in the subacromial space(considered the 'roof' of the shoulder blade) is pinched.
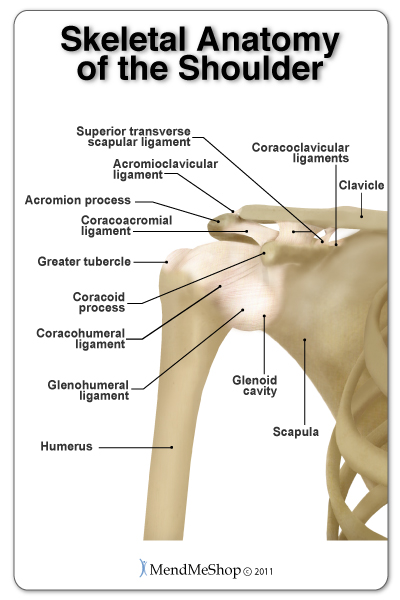
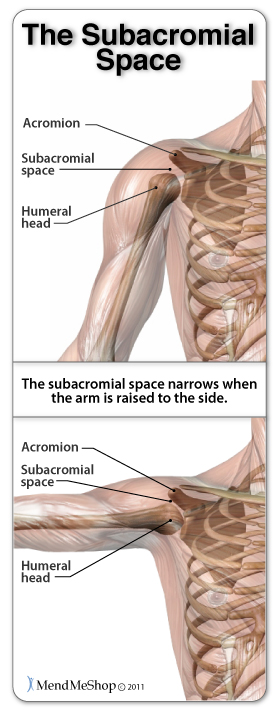
The subacromial space is an area in the shoulder that's approximately 1/2 an inch wide between the humerus (upper arm bone) and the acromion (a boney projection of the scapula).As you raise your arm, the greater tubercle (head of the humerus) moves up towards the acromion process and the amount of space in the subacromial space is naturally reduced. When the shoulder is healthy and everything is functioning properly this narrowed space is not a problem.
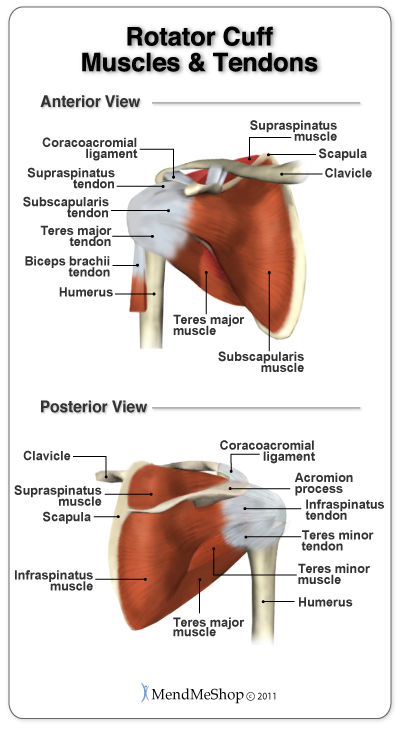
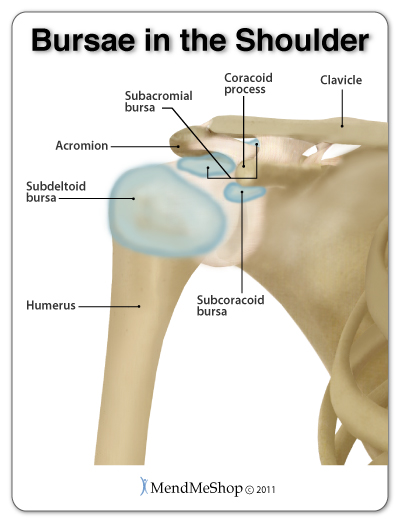
The supraspinatus tendon and thesubacromial bursa lie within the subacromial space. Therefore, these tissues are at the greatest risk of being pinched between the humerus and acromion process when you lift your arm. If the soft tissue in the subacromial space is swollen or the acromion is abnormally shaped, pinching or rubbing of the supraspinatus tendon may occur and/or it can cause a lot of irritation in the subacromial bursa. This pinching of the supraspinatus tendon or subacromial bursa causes the pain of shoulder impingement syndrome, which becomes worse as inflammation increases.
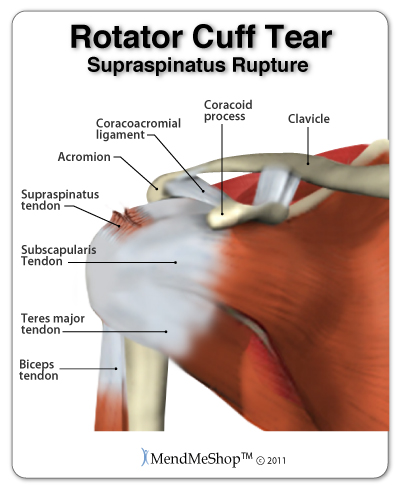
Abnormal narrowing of the subacromial spacecan happen as a result of bone spurs, thickening or calcification of the coracoacromial ligament, a curved or hooked acromion, a misaligned glenohumeral joint, or osteoarthritis spurs on the acromioclavicular joint. Alternatively, if the soft tissue within the space is larger than normal the space becomes even more narrow. This can occur with subacromial bursitis, or swelling orthickening of the supraspinatus tendon.
This condition is also referred to as swimmer’s shoulder, pitcher's shoulder, painful arc syndrome, supraspinatus syndrome, and thrower's shoulder. Because it can mimic the symptoms of a rotator cuff tear, tendonitis, tendosynovitis, bursitis or other shoulder problems, it is wise to see a doctor to determine the cause of your shoulder pain.
Symptoms of Shoulder Impingement Syndrome
Typical symptoms of impingement syndrome are the gradual development of shoulder pain over time.
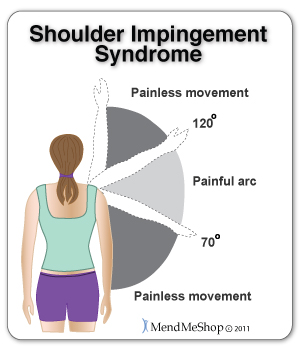
Pain usually occurs when reaching behind your back (internal rotation) or when lifting your arm. As you raise your arm, the pain is noticeable between 70° and 120°, but not when your arm is straight up or pointing down. This is because when you begin to raise your arm (abduction) there is no pinching, but during the lift, the top of thehumerus moves closer to the acromion, limiting the space.
With an external impingement, you with feel pain at the front and/or side of the joint when making a throwing motion.
If you experience pain when holding your arm out to the side (abducted) or turning it outward it would indicate you have an internal impingement.
3 Stages of Shoulder Impingement
There are three distinct stages of shoulder impingement that all have different symptoms.
Stage I
In stage I of impingement you will feel a
slight ache after repetitive overhead movements. Inflammation will occur within the joint but at this stage it can be treated. Treating the pain and inflammation with
cold compression will help to reduce inflammation and swelling. However, if the impingement is caused by an abnormal bone growth or misaligned joint, the cause may need to be fixed with surgery to
avoid the impingement from continuing.
Stage II
Stage II of impingement is when the inflammation has progressed and scar tissue starts to form on the supraspinatus tendon and subacromial bursa. This makes the tissue thicker and more prone to further injury. As the tendon and bursa become thicker and more susceptible to impingement, it becomes difficult to break the cycle.
During stage II you will experience more pain when doing overhead activity and possibly while sleeping. It isimportant to treat the scar tissue and inflammation to prevent more chronic problems and to perform appropriate exercises, that will not pinch the supraspinatus tendon or subacromial bursa, tomaintain as much range of motion as possible.
Stage III
Stage III of impingement progresses to the stage where abnormal bone formations cause further complications. The subacromial space can be limited by bone spurs, calcification of the supraspinatus tendon, and even osteophytes (small bone growths) that grow on the acromion and/or head of the humerus. This restricts the space available for the tendon to pass through the subacromial space even more, creating stiffness, lack of mobility in the shoulder, and lots of pain.
At this stage, surgery may be one of the only options in order to remove the bony formation, and return to a normal range of motion and less pain in the shoulder.
Diagnosis
Visiting your doctor when you have shoulder pain is always recommended, as there are many possible causes of shoulder pain. Sometimes, one set of symptoms can result in multiple diagnoses. An x-ray and a MRI are often needed in order to diagnose a shoulder ailment properly.
A test for shoulder impingement syndromeis to reach the affected arm behind you towards your lower back, as if to get something out of your back pocket. If you feel sharp pain with this motion, it is possible you have shoulder impingement syndrome and you should see your doctor.
You doctor may refer you to a physical therapist. Many people see great improvements in physical therapy with shoulder related problems and are able to treat the condition with conservative measures such as cold compression, and Blood Flow Stimulation Therapy™.
Causes
- Tendonitis of the rotator cuff tendons
- Subacromial (shoulder) bursitis
- Genetic predisposition (small space between the acromion and humerus)
- Curved or hooked acromion
- Bone spurs in the shoulder
- Shoulder instability
- Biceps tendinopathy
- Other rotator cuff issues
- Dysfunctional shoulder blade (scapula) movement
Treatments - What You Can Do!
If you have shoulder impingement syndrome rest is highly recommended. Avoid activities that cause pain or may have caused the impingement and begin cold compression treatments as soon as possible.
The trick to healing your inflamed supraspinatus tendon and subacromial bursa is getting it to heal with minimal scar tissue - something the Shoulder Inferno Wrap® is great at! Without treating the scar tissue on the tendons and bursa in the subacromial space, thickening of the tissue can occur leaving you at risk. However, if you heal your shoulder impingement properly and treat scar tissue build up, your chance of recurring impingement or chronic shoulder conditions later on is much lower than average.
There are healing tools that can help treat your supraspinatus tendonitis and speed up the healing process so you can get back to a life without pain and risk of further injury. Blood Flow Stimulation Therapy (BFST®) will treat scar tissue and promote blood flow to heal your tendonitis faster and more completely than any other methods available.
Freezie Wrap® Cold Compression Therapy
To decrease inflammation and relieve the pain of shoulder impingement syndromedoctor's recommend cold compression therapy. Cold compression therapy willrelieve pain and swelling and will reduce, or even eliminate, the need for NSAIDs. Our Freezie Wrap® products, in our opinion, will provide you with the most effective Cold Compression Therapy available for the home market.
The
Shoulder Freezie Wrap® is the cold compression tool you need to treat your supraspinatus tendon, subacromial bursa and other shoulder tissue in an effective and convenient way.
Cold Compression Therapy works byinterrupting and slowing nerve and cell function in the injured area and reducing swelling that can block blood vessels. This is important because once blood vessels are blocked or damaged, they can no longer carry oxygenated blood through your tendon and tissue cells begin to break-down. Without cold compression therapy cellular break-down and tissue damage continues as the cells do not get the oxygen they need to survive. By limiting the amount of damage done to your supraspinatus tendon, you also limit the amount of healing that needs to occur. This is a very important step to get rid of shoulder impingement faster and with less pain!
The deep cooling effect provided by the Shoulder Freezie Wrap® not only reduces tissue damage, because the cold wraps gently numb the nerves the wraps alsoreduce pain!
The Shoulder Freezie Wrap® uses a supercharged cooling gel pack, that chills in the fridge, not in the freezer like ice or other freezer packs, giving you deep cold therapy without the risk of 'cold burns'or cryoburn. The medical-grade wrap keeps the cold directly off your skin preventing cryoburn while delivering cold right where you need it.
Inferno Wrap® Blood Flow Stimulation Therapy
After severe inflammation and swelling is reduced, begin treating your rotator cuff with Blood Flow Stimulation Therapy (BFST®). BFST® increases the amount of blood that flows naturally to your shoulder to nourish your subacromial bursa and supraspinatus tendon to speed healing.
The rotator cuff naturally receives a limited blood supply and when you stop moving your shoulder because it hurts the blood flow is reduced even further, limiting your body's natural ability to heal itself.
By treating your rotator cuff tendon with BFST®you can increase your body's blood supply to the shoulder and increase your body's natural healing power.
An Inferno Wrap® is the tool you need to treat your sore shoulder because it speeds healing and relaxes the surrounding muscles.
With BFST
®, tissues are safely and gently stimulated. Your body responds with a rapid increase in blood flow to the rotator cuff,
increasing the supply of oxygen and nutrients to injured tissue cells to promote healing. Our
Shoulder Inferno Wrap® provides
effective, non-invasive, non-addictive pain relief and healing with no side effects.
In addition, the improved blood flow whisks away dead cells and toxins that have built up from your damaged tendon and bursa. When you stop moving your arm and shoulder due to shoulder pain, your muscles and other tissue can become weaker and dead cells and toxins in the area can cause further tissue deterioration - this can lead to atrophy. By clearing the area of toxins and increasing the amount of oxygen and nutrients to your muscles and other tissue, the risk of atrophy (muscle weakness and/or deterioration) is greatly reduced. Keeping your upper arm, shoulder and rotator cuff tissue as healthy as possible throughout the healing process will allow you to improve shoulder strength again once your pain has gone and your shoulder impingement syndrome is gone.
Not only does the Inferno Wrap
® aid in reducing inflammation and improving healing, it helps to
prevent long term complications. Pain, lack of mobility, tendinosis, or a complete
rupture in the rotator cuff are some of the more common long term complications that can occur when shoulder impingement syndrome goes untreated. By treating your rotator cuff
with our BFST® device, scar tissue becomes softer and the supraspinatus tendon, subacromial bursa, and other tissue becomes stronger and more elastic,
reducing the risk of chronic problems in the future.
During the healing process, scar tissue builds on the supraspinatus tendon. This scar tissue can cause the tendon to thicken, decreasing the area in the subacromial space and increasing the chance of impingement.
In addition,
scar tissue can also bind the tendons and ligaments together within the joint capsule and surrounding the rotator cuff. The inflexible
scar tissue limits the movement of these tendons and ligaments that were once elastic and allowed the shoulder its large range of motion. As a result, movement of the entire joint is limited making it difficult to lift your arm or to reach for objects.
If left untreated, the shoulder may 'freeze' (a condition called
frozen shoulder or adhesive capsulitis) altogether making movement impossible. At the very least,
scar tissue leaves your tendon weaker than a healthy tendon, leaving your rotator cuff at greater risk of further deterioration and possible tearing.
Fortunately, you can treat your subacromial bursa and supraspinatus tendon with the ShoulderInferno Wrap® to soften scar tissue and improve the motion and flexibility of your shoulder.
Once the inflammation of your shoulder impingement has been reduced, nourishing and strengthening the supraspinatus tendon and surrounding area is recommended. Using Blood Flow Stimulation Therapy will speed your recovery and heal your rotator cuff more completely preparing it for strengthening exercises. Talk to your doctor or physical therapist to find out which exercises are appropriate for your situation.
With these simple and safe home treatment therapies - Freezie Wrap® cold compression therapy and BFST® therapy, you will notice significantly reduced pain and an incredible improvement in your rotator cuff range of motion.
Remember: We recommend that you consult your doctor and/or physiotherapist before using any of our outstanding products, to make sure they're right for you and your condition.
During your recovery, you may have to modify and/or eliminate any activities that cause pain or discomfort in your shoulder until your pain and inflammation settle and you gain more mobility and strength in your shoulder. The more diligent you are with your treatment and rehabilitation, the faster you will see successful results!
Surgery
Surgery for shoulder impingement is sometimes required to make more physical space for the supraspinatus tendon to slide. This can be done a number of ways; removing part of the acromion, making the space between the acromion and humerus physically larger, or removing the subacromial bursa. Your doctor or surgeon willdiscuss your options with you and talk to you about the procedures and what to expect from the surgery.
Recovery time for the surgery will depend a number of different factors including your healing ability, diet, rest, and the type of procedure done during surgery. Your doctor will advise you on your recovery, and will let you know if/when physical therapy can be started.
Following shoulder impingement surgery, using cold compression and and BFST® will shorten the time you require to heal. It addition, by treating the scar tissue that builds as your surgical site heals, your tendon, bursa and surrounding tissue will be healthier and more elastic to prevent future problems from developing.











 There are hundreds of kettlebell and bodyweight exercises, but that does not mean you should do them all. Too much variety creates an illusion of progress. Instead, concentrate on the most comprehensive and fundamental exercises. Most of your training should be
There are hundreds of kettlebell and bodyweight exercises, but that does not mean you should do them all. Too much variety creates an illusion of progress. Instead, concentrate on the most comprehensive and fundamental exercises. Most of your training should be  Kettlebell Renegade Row
Kettlebell Renegade Row